
Lens selection guide
Cataract surgery is very simply a lens exchange surgery. You are taking out your natural lens that has become cloudy and is distorting light, what we call a cataract, and inject an artificial lens (intraocular lens, IOL) made of plastic (acrylic or silicone). Decades ago before we had IOLs patients needed to wear very thick contacts or very thick eyeglasses (“Coke bottle” glasses). Fortunately, we can now place a lens inside the eye (IOL) at the time of surgery to replace the power lost when we remove the cataract. We try to match the power of the IOL to the optics of the eye. Therefore cataract surgery is a refractive procedure, and all ophthalmologists who perform cataract surgery are refractive surgeons.
Choosing a lens implant for cataract surgery can feel stressful and confusing. There are many different options, each with its own features, benefits, and costs. It is completely normal to feel overwhelmed by the amount of information and this decision. We understand that this choice is important, and that it can have a meaningful impact on your vision and daily life after surgery.
There are a lot of sources of information out there with different motives. There are now provocative Youtube videos of surgeons who tout specific products to become subject mater influencers. There also a financial incentive for industry and ophthalmologists to use certain lens types. Some practices utilize surgical counselors who have influence over the information you receive relative to lens selection. Then there are also friends and family who have their own anecdotal experiences with lenses.
To be clear we all have our own biases. This can even relate to how we view price being related to quality. Our practice’s goal is to be as objective as possible and to guide you through each option clearly and thoughtfully, so you feel informed and confident in your decision. Cataract surgery is not a one-size-fits-all experience; every patient has unique vision needs, daily activities, and expectations. We try to take the time to listen, explain your choices, and help you select a lens implant that aligns with your lifestyle and visual goals.

What is refractive error?
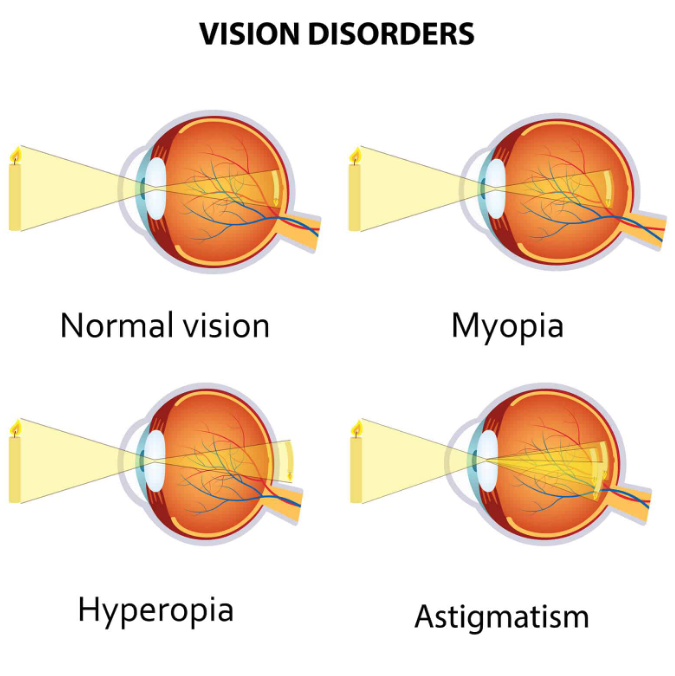
Any discussion of cataract surgery and IOLs has to discuss refractive error. Refractive error is a common vision condition that occurs when the eye does not bend (refract) light correctly to focus it precisely on the retina—the light-sensitive tissue at the back of the eye responsible for clear vision. When light is not focused accurately, images appear blurry or distorted.
In a normally shaped eye, light rays enter through the cornea and lens and are brought into sharp focus directly on the retina. In refractive error, this process is disrupted due to the shape of the eye, the curvature of the cornea, or the focusing power of the lens. This causes light to focus in front of the retina (myopia/near sightedness), behind the retina (hyperopia/farsightedness), or at multiple points (astigmatism), rather than at a single, clear focal point. As a result, vision may be blurry at distance, near, or both. Refractive error can be corrected with glasses or contacts, or surgically with corneal refractive surgery (PRK, LASIK, or SMILE). Generally when we get older and we have cataract findings in our lenses that limit vision even with glasses and contacts we recommend cataract surgery, which can be refractive because of the choice of power and lens type in intraocular lens implants.
What is astigmatism?
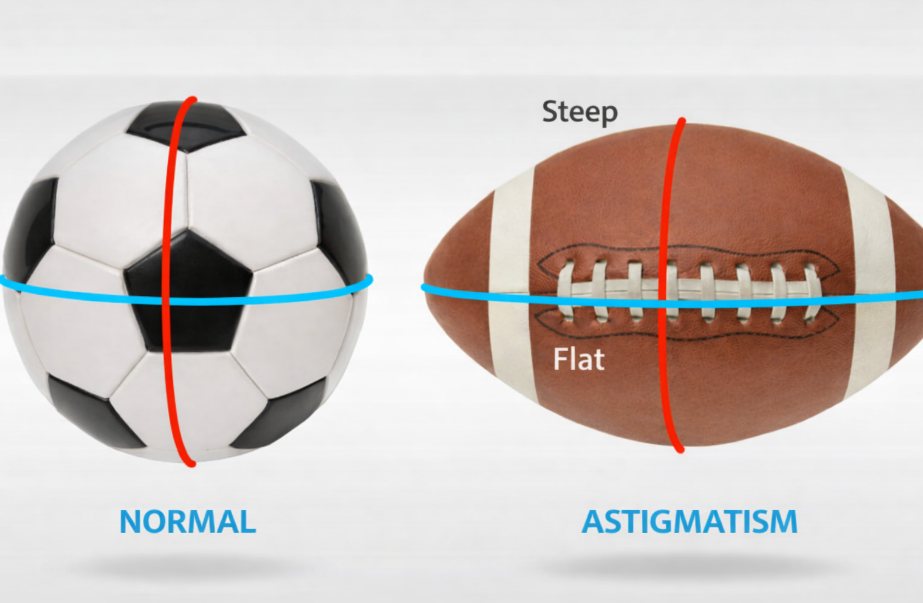
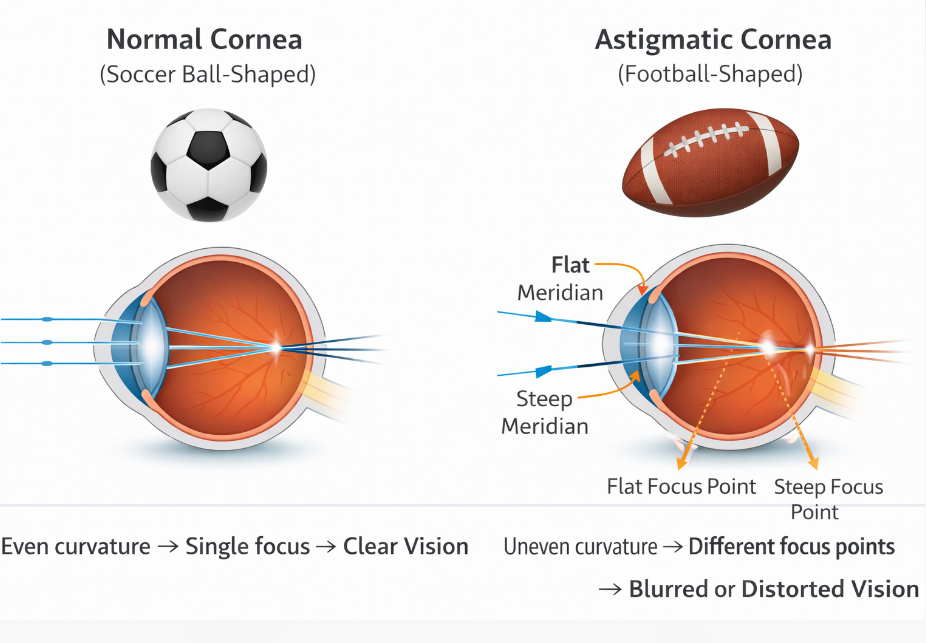
Astigmatism is a type of refractive error in which the eye does not focus light to a single, sharp point on the retina, resulting in blurred or distorted vision at both distance and near. This occurs because the eye has different focusing power in different directions, rather than being evenly curved like a smooth sphere. Instead of light rays coming together at one focal point, they focus at multiple points, creating image blur or shadowing.
Regular astigmatism—the most common form—can originate from either the cornea or the natural lens inside the eye, or a combination of both.
Corneal astigmatism occurs when the front surface of the eye is shaped more like a football than a basketball, with one meridian steeper than the other.
Lenticular astigmatism arises from asymmetry in the curvature or position of the eye’s internal lens.
In both cases, the principal meridians are perpendicular to each other, which allows regular astigmatism to be effectively corrected with glasses, contact lenses, or specialized intraocular lenses during cataract surgery.
A monofocal lens
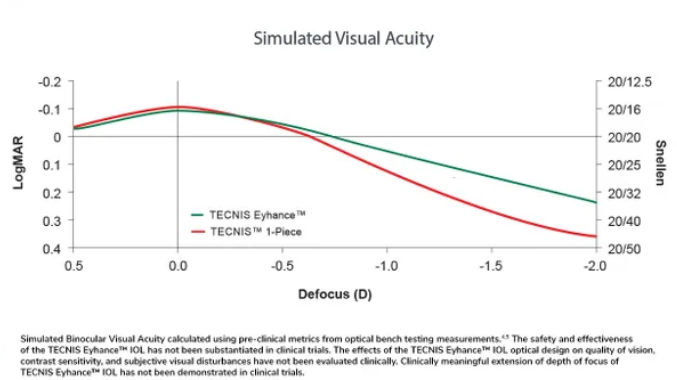
Monofocal intraocular lenses (IOLs) are the tried-and-true standard for cataract surgery and have been safely used for several decades. They are designed to provide clear vision at a single focal point—most often set for distance—offering reliable, predictable results. Because they have been around for so long, surgeons have extensive experience with them, and their performance and safety profile are well understood. For many patients, this long track record makes monofocal IOLs a trusted choice, delivering consistently good clarity of vision with minimal visual side effects. However, these lenses have continued to evolve and improve over the years. We opt to use the Johnson and Johnson “Eyhance” monofocal lens, which is an excellent lens that provides some extended range of vision (please see the inserted graph).

What a monofocal IOL does well
A monofocal lens is designed to give clear vision at one primary distance, most commonly far (distance) vision. After surgery, many patients:
See clearly for driving, watching TV, and recognizing faces
Experience sharper, brighter vision than before surgery
Have reliable, high-quality vision with excellent contrast
Monofocal lenses are the most commonly used IOLs and are considered the gold standard for optical clarity and predictability.
What it does not do
Because it focuses at only one distance:
Reading glasses are usually needed for near tasks (reading, phone use)
Computer or intermediate glasses may be needed depending on how the lens is targeted
Astigmatism may still blur vision unless it is corrected with glasses, a toric lens, or surgical techniques
Vision quality expectations
With a monofocal IOL, patients typically experience:
Minimal glare or halos
Very stable vision
Excellent night vision compared to multifocal lenses
This makes monofocal lenses especially appealing for patients who:
Prioritize crisp, dependable vision
Drive at night frequently
Want the lowest risk of visual side effects
Bottom line
Yes — you can see very well with a monofocal IOL, especially for distance vision. While it does not provide a full range of vision without glasses, it delivers high-quality, dependable eyesight and remains an excellent choice for many cataract patients.
If you’d like, I can also explain:
Monovision with monofocal lenses
How astigmatism affects results
How monofocal lenses compare to premium lenses
What daily life typically looks like after surgery
“Standard” vs “Premium” lenses
Monofocal lenses are the lenses covered by insurance, and therefore some practices may refer to them as “standard lenses” or lenses paid for by “the government”. This terminology can be misleading especially when framing the discussion in terms of “standard” lenses vs “premium” lenses which patients have to pay extra for. Patients can infer with the terminology that they will they get an inferior product placed in their eye if they opt for a standard lens. However, this is not true. We would not implant them if they did not. If you eye is healthy, everyone who has cataract surgery with a monofocal lens will have the ability to see 20/20 and notice a large improvement in their visual potential after cataract surgery.
Using terminology like “premium” vs “standard” and then pricing accordingly, is also part of a marketing strategy called “price premium” which is meant to signal to potential patients that if they spend more they will get a better product. This can make people feel like if they opt for the standard lens they are choosing a Yugo car versus a Mercedes. However, this analogy is not correct. Monofocal lenses provide excellent optics. The real question is how will you see without glasses and that is where the discussion of “premium” vs “standard” lenses comes in. So the analogy is more between a Mercedes convertible versus a sedan. Both quality products, the question is how do you want to experience driving. In a similar way the question is how do you want to experience seeing with or without glasses.
Believe it or not there are situations where a “standard” lens are better for the patient than paying up for a “premium” lens. We discuss some of those scenarios in the FAQ in this section.


What is Monovision?
Monovision is a vision strategy commonly used in cataract surgery or refractive procedures in which each eye is set to focus at a different distance. Typically, one eye is optimized for distance vision, typically the dominant eye, while the other is optimized for near vision. The brain learns to blend the input from both eyes (neuroadaptation), allowing many people to see well at multiple distances without relying as much on glasses. Monovision can be an effective option for reducing dependence on reading glasses, but it requires adaptation and may slightly reduce depth perception or clarity at certain distances. Not everyone tolerates monovision equally well, which is why the amount of difference between the two eyes is carefully tailored to each patient. Patients who have successfully neuroadapted already to monovision by wearing contacts or having corneal refractive surgery are excellent candidates for monovision at the time of cataract surgery. This will allow them to use standard monofocal lenses or toric monofocal lenses to help them achieve eye glasses independence. We try to be conservative in monovision, using micro or mini monovision, when patients have not experienced monovision before. Even micro or mini monovision will give patients a degree of independence from eyeglasses after surgery, especially when using monofocal lenses with extended depth of focus.
Micro monovision uses a very small difference in focus between the two eyes, usually around 0.50 diopters or less. The goal is to provide a subtle boost in near or intermediate vision while preserving excellent distance vision in both eyes. Because the difference is minimal, most patients adapt easily, with little impact on depth perception or visual quality. This approach is often chosen by patients who prioritize crisp distance vision but want some added flexibility for tasks like computer work or occasional reading.
Mini monovision creates a moderate difference between the eyes, typically around 0.75 to 1.25 diopters. This provides greater near vision support than micro monovision while still maintaining good distance vision in both eyes. Many patients find this a good balance between spectacle independence and visual comfort. Mini monovision may slightly affect depth perception, but most people adapt well and appreciate the increased range of vision for everyday activities.
Standard monovision involves a larger difference between the two eyes, usually 1.50 to 2.50 diopters or more. One eye is clearly dedicated to distance vision, while the other is dedicated to near tasks such as reading. This approach offers the greatest reduction in dependence on reading glasses but can come with more noticeable trade-offs, including reduced depth perception, contrast sensitivity, or overall visual sharpness. Standard monovision requires more adaptation and is best suited for patients who strongly prioritize near vision and are comfortable with the compromise.
Frequently Asked Questions about monofocal lenses and monovision
-
It depends on what distance you are looking for and if you have astigmatism. If you have astigmatism, and you elect to not fix it with a toric lens, at the time of surgery, then you will have some residual blurry vision after cartaract surgery that will have to be sharpened with glasses or contacts. Also keep in mind that a monofocal lens is set for one distance, so you will see your best without glasses at that distance, but you will not see well at other distances. For example, if you elect to see in the distance with a monofocal lens, your near and intermediate vision will not be as clear.
-
There are a few situations where a monofocal lens is preferable than paying extra out-of-pocket for a “premium lens”.
you have pre-existing eye disease such as macular degeneration, advanced glaucoma, fuchs corneal dystrophy, or other eye disorder. A toric lens may still be helpful if you have moderate to large amounts of astigmatism, but multifocal lenses should generally be avoided in these situations, as visual quality can actually be worse with a multifocal lens if you have these conditions than with a monofocal lens or simple toric lens.
You don’t mind wearing glasses. That is okay. Some people view glasses as part of their “look” and also prefer to wear progressive eyeglasses that help with reading and near vision anyways. They don’t want to have to put on and take off reading glasses. They would just prefer to wear glasses all the time.
You don’t have the means to pay for the extra cost of a “premium” lens. Please rest assured that is okay. You will see much better after cataract surgery and have the ability to fine tune your vision with glasses or contacts after surgery.
-
Because a monofocal lens has one focal point. It will only be focused at one distance. Most patients opt to have their vision wtihout glasses optimized for distance vision, but some people choose to focus their eyes for intermediate or near vision.
-
Overall, we would suggest that continuing with monovision is a good idea once your brain has already neuro adapted to it.
-
Yes he can certainly have monovision even if you have never experienced it before with contact lenses or refractive surgery. In fact we do believe having some under correction in the non-dominant can be useful for functional vision without glasses for everyday tasks like looking at your watch or phone. However we do feel is advisable to stick to mini or micro monovision if you have never experienced it before.
Toric lens implants
A toric lens implant is a specialized intraocular lens designed for patients who have cataracts and astigmatism. Not everybody has corneal astigmatism and in these patients a standard monofocal lens can neautralize most of their refractive error, near sightedness (myopia) or far-sightedness (hyperopia), at the distance they desire. In some patients with a previous diagnosis of astigmatism, most of their astigmatism is actually in their lens/cataract. Therefore, when they have cataract surgery, their astigmatism will be fixed just by removing their cataract. However, for those people who have corneal astigmatism, a toric lens can help give them a degree of eyeglasses independence after their cataract surgery.
A toric lens has unique markings in one axis. These markings are used during cataract surgery, to precisely align the toric lens inside the eye to neutralize corneal astigmatism. Toric lenses are also manufactured as multifocal lenses. If a person has corneal astigmatism a monofocal or multifocal toric lens can significantly improve their vision without glasses. We use the Johnson and Johnson toric lens portfolio for monofocal torics because of the extended depth of focus of the Eyhance platform. We also appreciate the stability fo the lens.

Multifocal or Extended Depth of Focus Lenses
Multifocal intraocular lenses (IOLs) and Extended Depth of Focus (EDOF) IOLs, are premium lens implants used at the time of cataract surgery to reduce dependence on glasses by providing vision at more than one distance. Multifocals provide good vision at distance, intermediate, and near. EDOF lenses tend to focus more on distance and intermediate. These lenses split incoming light into multiple focal points, allowing the brain to select the image it needs for different viewing tasks. While these lenses offer more full range of vision using one eye, there are also some trade-offs in vision that have to be understood and accepted. Below is a brief summary of some of the good and bad of these lenses.
Pros of Multifocal and Extended Depth of Focus (EDOF) IOLs
Reduced dependence on glasses for daily activities
Improved range of vision, including distance, intermediate (computer), and sometimes near
Convenience and lifestyle freedom, especially for active patients
EDOF lenses (e.g J&J Symphony lens) often provide:
Better night vision quality than traditional multifocals with fewer halos and glare for many patients
More forgiving refractively for patients with any residual refractive error after surgery
Multifocal (e.g J&J Odyssey lens) lenses.
More range of vision from distance to near with one eye.
Cons of Multifocal and EDOF IOLs
Halos, glare, or starbursts, especially at night (more common with traditional multifocals)
Reduced contrast sensitivity, particularly in low-light conditions
Neuroadaptation period—the brain may take weeks to months to adjust
Not ideal for all eyes, especially those with existing ocular disease:
Significant dry eye
Retinal disease (e.g., macular degeneration)
Irregular corneas or prior refractive surgery
EDOF lenses may still require:
Reading glasses for fine print or prolonged near work

The Light Adjustable Lens (LAL)
We are proud to be one of the first practices to offer the light adjustable lens (LAL)
The LAL is the only intraocular lens (IOL) placed at the time of cataract surgery that can be adjusted after surgery. It is the most precise way to have cataract surgery. The lens has been in development for over 20 years and is based on noble prize winning polymer chemistry research from CalTech. The lens is manufactured by RxSight, which is based in Orange County California. The LAL was approved by the FDA in 2017 and became available for practices to use in 2019. To date, over 30,000 lenses have been implanted. We began using the LAL in 2021.
How is the LAL different?
With all other IOLs used in cataract surgery we try to provide the best possible vision we can. However, there are limits to how accurate we can be because we are making estimates based on your pre-operative testing. Remarkably, the LAL’s shape is changed in your eye after surgery by using a specific frequency of UV light. By changing the shape of the lens in your eye after surgery, we are able to customize your vision after surgery.
After surgery a patient will have 3 to 5 light treatments over 2 to 3 weeks to change the power of the lens and lock-in that power in their eye. The treatments average 90 seconds, but the visits can last 1 hour as they require a refraction and dilation. This treatment takes place in our office, where we have a light delivery device that can change the lens power. Leading up to a patient’s final treatment (lock-in), patients will need to wear UV protecting eyeglasses, that the company provides, to prevent changing the power of the lens from inadvertent UV light exposure.

Frequently Asked Questions and the Light Adjustable Lens (LAL)
-
Customized vision is important because it allows us to provide the most precise post operative vision without glasses and also to customize how a patient wants to see. With traditional intraocular lenses (IOLs), a patient is relying on their surgeon to predict how they want to see after surgery. With the LAL, a patient will tell us how they want to see and what they want to see without glasses. It shifts the control of uncorrected visual acuity from the doctor to the patient. If a patient wants more uncorrected distance, intermediate, or near vision they can control that. Another way of thinking about the LAL, is that it is the difference between an off the shelf suit versus a tailored suit.
-
For patients who want spectacle independence after cataract surgery in both eyes, the LAL system is very compelling. Greater than 80% of patients report that they do not need glasses after surgery. This precision approaches the results found with LASIK. The outcome results are higher than the 40 to 50% of patients who have eyeglass independence when traditional intraocular toric lenses are used.
Eyeglass independence is achieved through four mechanisms. First, the lens itself has an extended depth of focus, especially when adjusted with light to a near target. Secondly the lenses are adjustable in your eye. Thirdly, the lenses are typically adjusted to a small degree of monovision, which means that your dominant eye is set for distance and your non-dominant eye is set for intermediate/near. The degree of this difference is customized by the patient their visual preferences. Lastly, the lenses can be adjusted in 0.25 diopter steps vs a traditional intraocular lens that can only be chosen in 0.5 diopter steps. This leads to greater precision.
The LAL offers spectacle independence to more patients that may not qualify for a multifocal lens due to pre-existing disease or that may want to avoid some of the night-time symptoms experienced with multifocal lenses.
-
Anyone who is very motivated to have the most precise and clear vision after cataract surgery without glasses.
-
A patient’s pupil needs to dilate large enough for light treatments. This is generally 6 mm. Unfortunately, some patients will not dilate enough and will not qualify. Also, patients who may have previously had certain viral corneal disease or on photosensitizing medications that cannot be stopped should avoid the light treatment process. Most importantly, anyone who feels that they will not comply with wearing UV protection glasses at all times after surgery until their final light treatment, should not have the intraocular lens placed. Some patients may also have transportation issues and the increased number of post-operative visits and time may be difficult.
-
Fortunately, all is not lost if a patient forgets to wear their glasses for short periods of time. This is due to a special UV blocking layer on the lens called Optishield. This does provide protection, but until there are formal changes in protocol, we still recommend that patients wear their post-operative glasses at all times. Hopefully, as more data is collected about Optishield, we may be able to avoid wearing UV glasses indoors after surgery.
-
We charge $1,900 an eye for the lens. The lens costs more because it costs more than a traditional lens from the manufacturer. We also have to purchase the light delivery device for the office to treat the lenses.
However, you will likely want to adjust your lens. You can adjust your lens up to 3 times, but most people will only need to adjust their lens 1 or 2 times. Each treatment is $750. This is because each treatment visit lasts about 1 hour and the LDD device is needed to treat the lens and customize it to your eye.
Frequently Asked Questions and the Light Adjustable Lens (LAL)
-
We offer a range of solutions designed to meet your needs—whether you're just getting started or scaling something bigger. Everything is tailored to help you move forward with clarity and confidence.
-
Getting started is simple. Reach out through our contact form or schedule a call—we’ll walk you through the next steps and answer any questions along the way.
-
We combine a thoughtful, human-centered approach with clear communication and reliable results. It’s not just what we do—it’s how we do it that sets us apart.
-
You can reach us anytime via our contact page or email. We aim to respond quickly—usually within one business day.
-
We offer flexible pricing based on project type and complexity. After an initial conversation, we’ll provide a transparent quote with no hidden costs.
-
Collaborative, honest, and straightforward. We're here to guide the process, bring ideas to the table, and keep things moving.
Click on the picture to the right to test out a vision simulator of different lens types
Johnson and Johnson has a vision simulator that you can use to see what different lens types might be like with out glasses (click here or the image above)